Cases Study
▍Introduction
Before entering the field of digital implant dentistry, most clinicians begin by learning to use static surgical guides for implant placement. The workflow is intuitive and straightforward. Essentially, as long as a CBCT dataset is available, clinicians can design and print the guide themselves or outsource it to a dental laboratory with ease.
For this reason, static guided surgery remains the mainstream approach in digital implant workflows today.
▍Frequently Asked Questions in Courses
However, in my courses and lectures—often focused on complex implant planning or full-mouth reconstruction—clinicians frequently ask about the advantages and disadvantages of static guided surgery versus dynamic navigation.
Those who raise these questions are usually experienced implant clinicians who may have encountered certain limitations while using surgical guides.
Having accumulated substantial clinical experience with both static guides and dynamic navigation, I would like to share a brief comparison based on my personal observations.
▍Static Guides: Emphasis on Fit and Stability
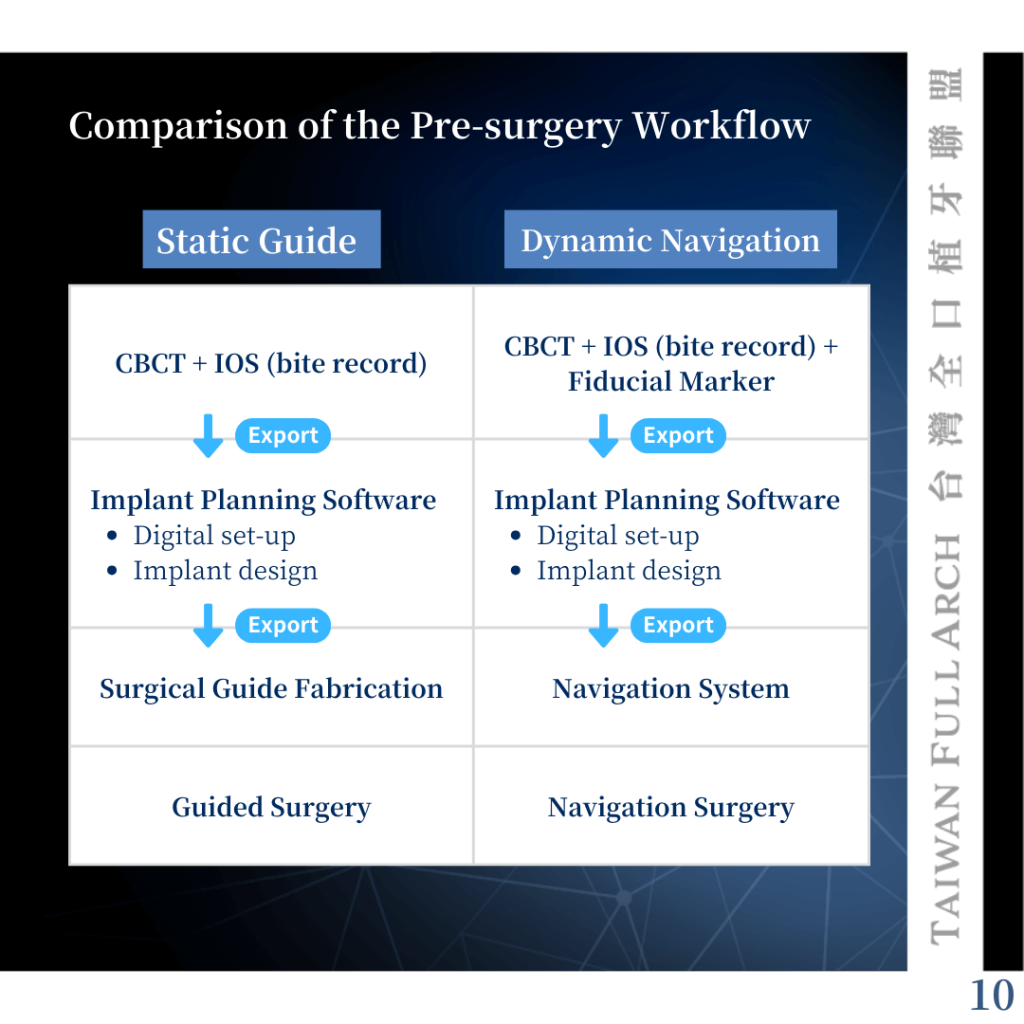
In fact, the preoperative workflow for both approaches is quite similar. Both require the integration of CBCT data and intraoral scans for prosthetic planning and implant positioning.
For static guided surgery, the key factor is the stability of the guide. Therefore, clinicians must carefully assess, prior to surgery, whether the guide may be unstable. For example, free-end guides or soft tissue–supported guides tend to have questionable stability and may require additional fixation devices, such as surgical guide pins.
▍Dynamic Navigation: Reliance on Three Reference Points
Dynamic navigation, on the other hand, depends on three stable and reproducible reference points. Clinicians must first confirm that three clearly identifiable landmarks can be found on intraoral hard tissues—typically distinct anatomical features on teeth, such as cusp tips, pits, and fossae.
If the teeth are unstable or in edentulous cases, additional fiducial markers (commonly mini screws) are required. Although the overall preparation is similar, each method has its own critical considerations.
▍Intraoperative Considerations Are Fundamentally Different
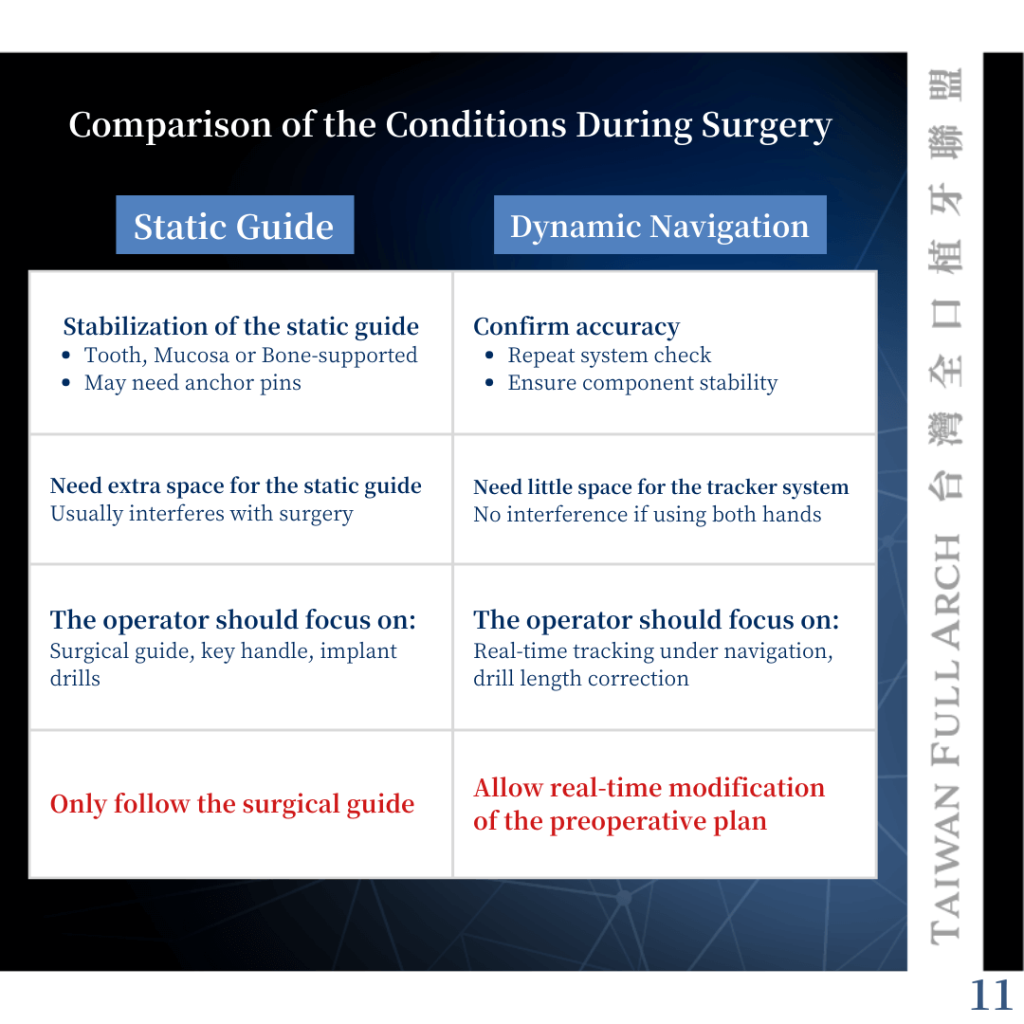
The key intraoperative concerns differ significantly between the two approaches.
With static guides, the primary focus is ensuring the stability of the guide throughout the procedure. In contrast, dynamic navigation requires continuous verification of the system’s accuracy.
This highlights a major difference: with a static guide, it is difficult to assess accuracy during surgery, whereas with dynamic navigation, accuracy can be monitored in real time. This greatly influences the clinician’s confidence in proceeding with the procedure.
▍Static Guides Follow; Dynamic Navigation Adjusts
During surgery, the points of attention also differ. Static guided surgery requires careful monitoring of the guide, guide components, and drills. Dynamic navigation requires attention to the drill position in relation to the 3D anatomical display and depth indicators on the screen.
In my opinion, the most critical difference is this: static guides can only be followed—regardless of whether they are correct or not—whereas dynamic navigation allows real-time correction and adjustment.
▍Differences in Surgical Field and Working Space
There are also significant differences in surgical visibility and working space. Static guides are often difficult to use in patients with limited mouth opening, whereas dynamic navigation does not restrict the surgical field.
However, dynamic navigation systems require a tracker, which is typically attached to the contralateral (non-operative) side. Therefore, clinicians should ideally be comfortable using both hands to avoid limitations during surgery.
▍Static Guides Require Favorable Bone Conditions
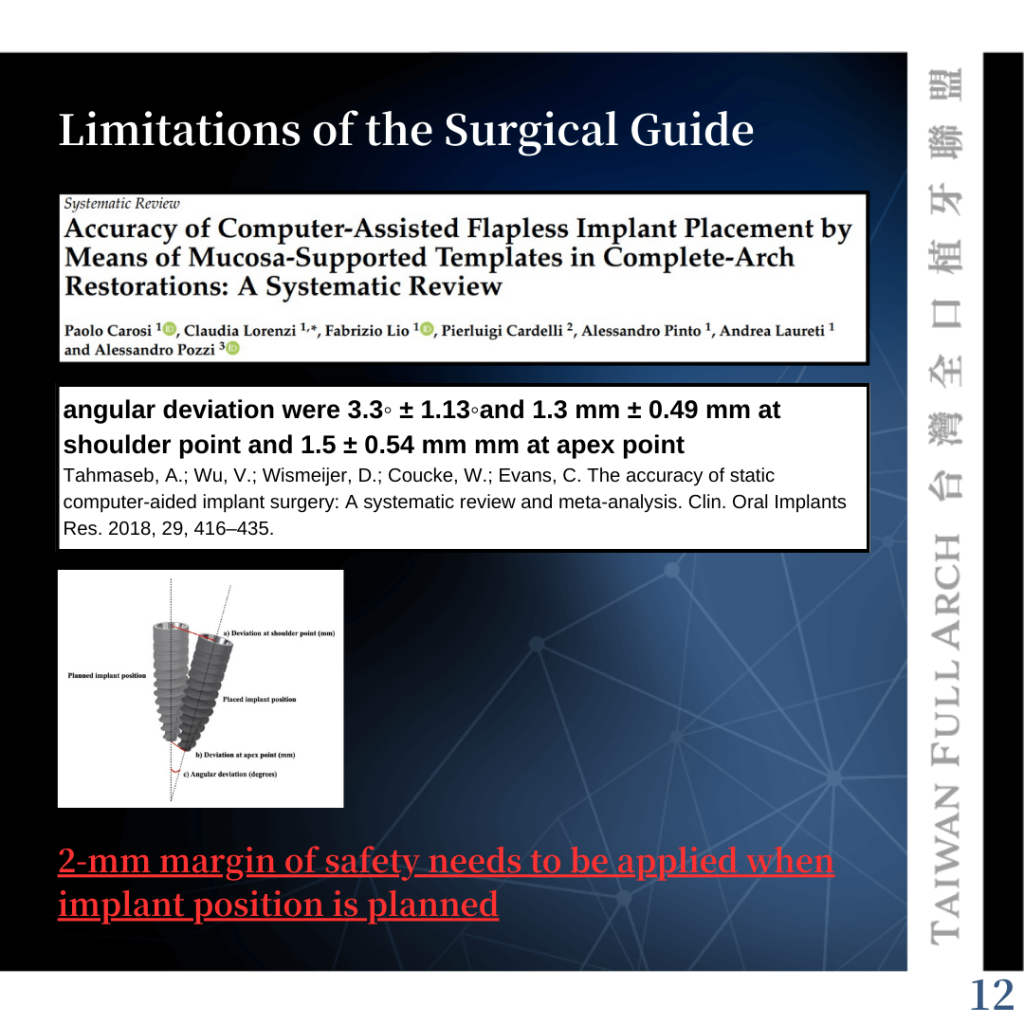
Based on selected literature, static guides are generally more suitable in cases with favorable bone conditions—specifically, when there is more than 2 mm of bone width in all dimensions.
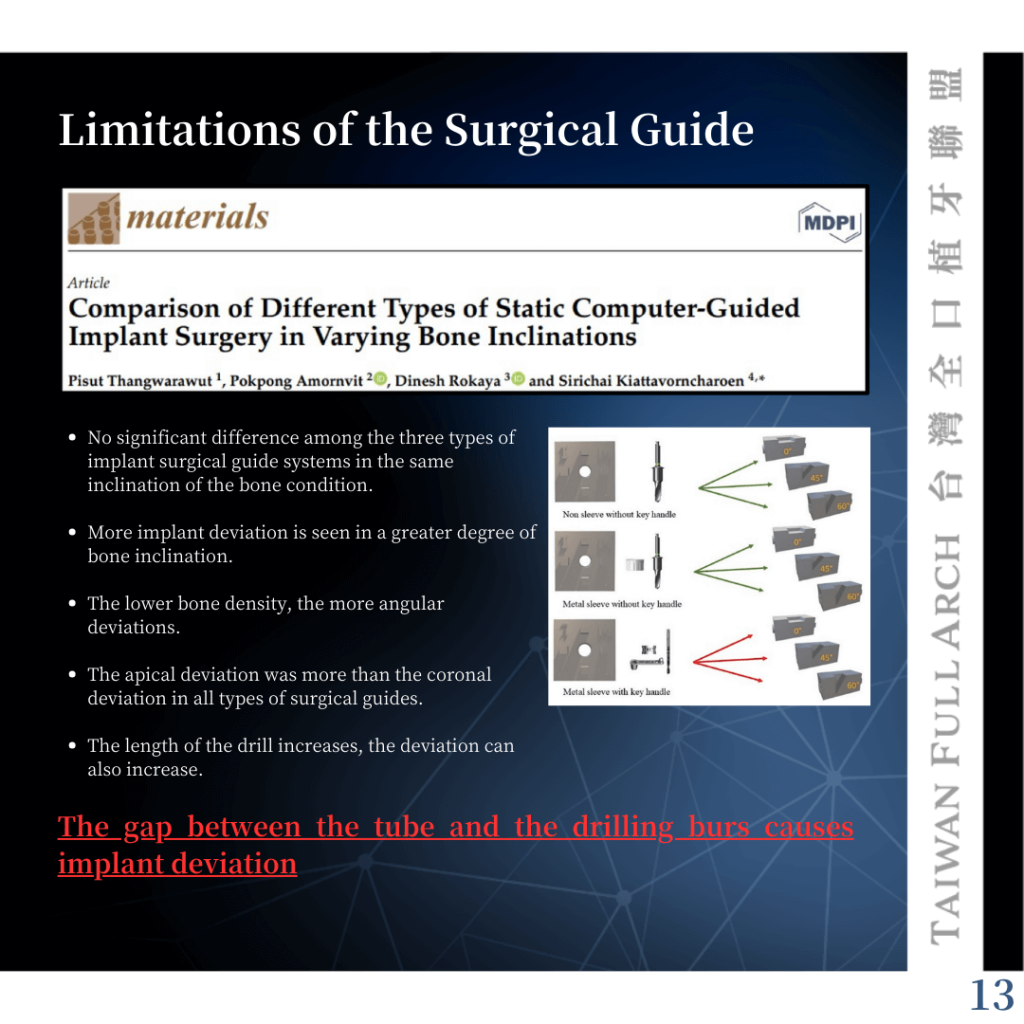
This is because multiple sources of error can accumulate throughout the workflow, and there is no opportunity for intraoperative correction, potentially leading to suboptimal outcomes.
This issue becomes especially pronounced when the bone surface is inclined. For example, in immediate implant placement in the anterior region, static guides may result in a buccal deviation of the implant. In contrast, dynamic navigation allows for overcorrection to compensate for such anatomical challenges.
▍Higher Long-Term Benefits of Dynamic Navigation
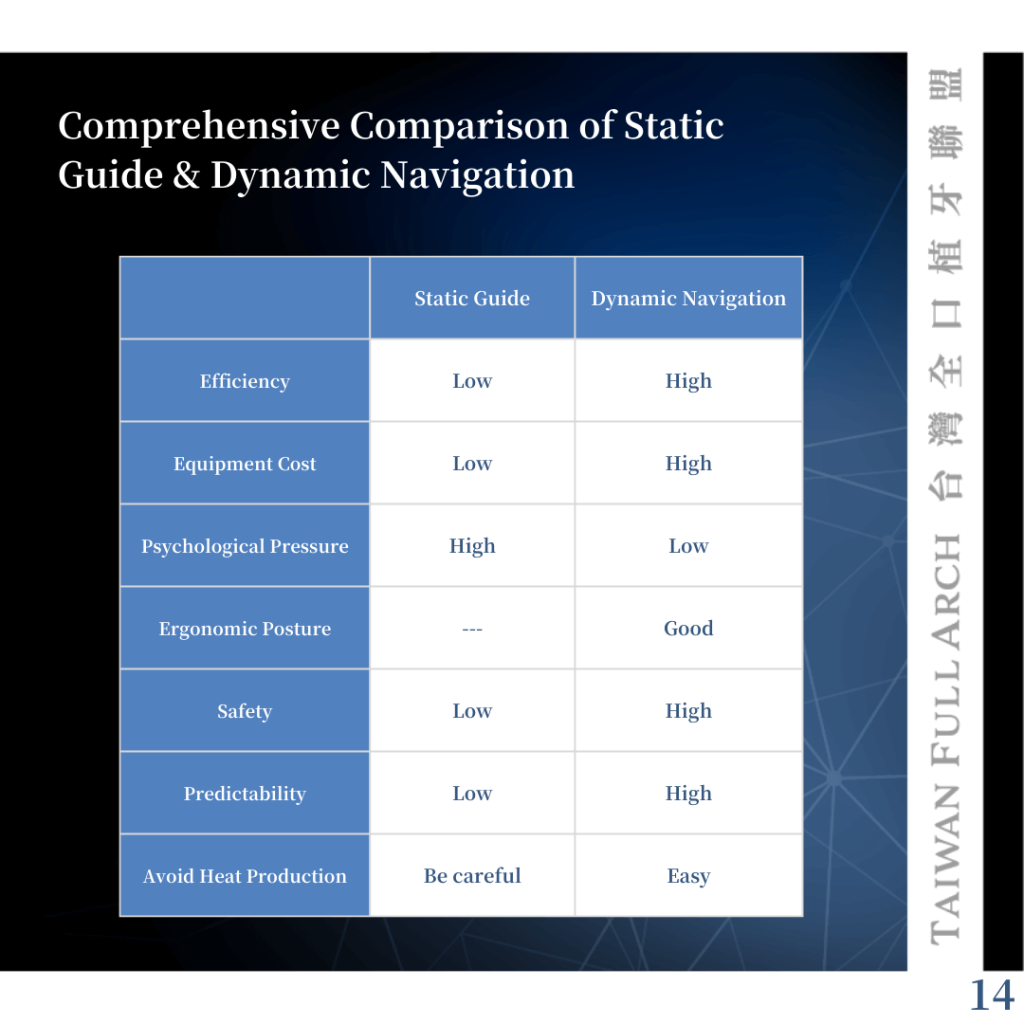
From an overall perspective, dynamic navigation requires a higher initial investment but offers greater long-term benefits.
In particular, it has significantly improved my surgical ergonomics and posture. While the accuracy of navigation systems remains a topic of debate, and the learning curve varies among clinicians, the advantages are evident.
If the goal is to reduce physical strain caused by poor posture and to achieve truly adaptive, real-time digital treatment, dynamic navigation is a modality worth serious consideration.
▍The Importance of Fundamental Surgical Skills
Ultimately, a thorough understanding of 3D anatomical structures and proficiency in freehand surgery are essential to fully utilize both static guides and dynamic navigation.
Before entering the digital realm, clinicians must first build strong fundamental surgical skills. Otherwise, reliance on digital tools may obscure critical clinical judgment.