In cases of terminal dentition or an edentulous ridge, if the goal is to avoid multiple surgeries and waiting periods associated with bone grafting and soft tissue grafting—while still achieving immediate function—the implant design should incorporate the PATZI implant protocol from the outset.
P: Pterygoid implant
A: Anterior or axial implant
T: Tilted implant or trans-sinus implant
Zi: Zygoma implant
This is especially important in the maxilla, where anatomical challenges are more complex. In many cases, utilizing all available treatment options is necessary to successfully complete the rehabilitation.
This case involves a female patient in her 50s with a smaller body frame and limited mouth opening, requiring only maxillary rehabilitation. Under these conditions, this is not an ideal indication for zygoma implants. Therefore, during treatment planning, priority should be given to alternatives to zygoma implants, reserving them only when no other options are feasible.
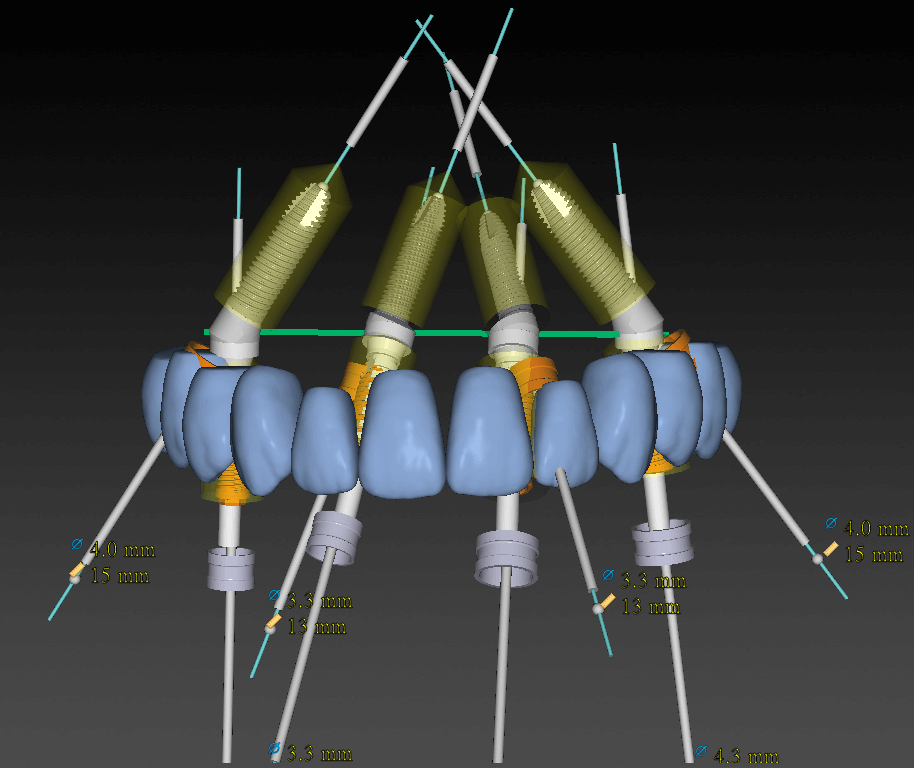
To maximize the AP spread, a trans-sinus implant was placed at the #15 position, while tilted implants were utilized in other areas.

Trans-sinus implants are often a challenging option for many clinicians. This is because, whether performing a sinus crestal approach or a lateral window approach, the sinus membrane is typically elevated from the inferior aspect upward. In contrast, sinus preparation for a trans-sinus implant is performed at an oblique angle.
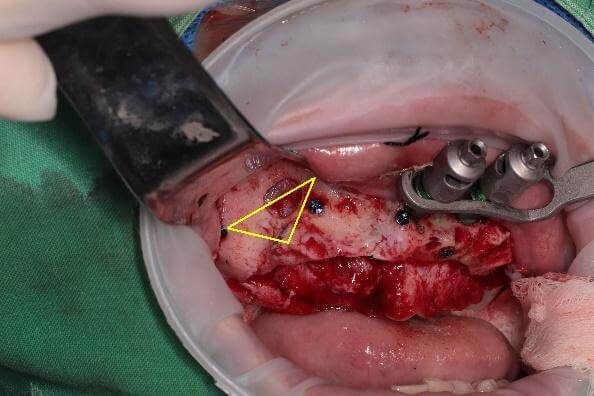
The key step is opening the anterior wall of the sinus (which I refer to as the “trans-sinus big triangle,” indicated by the yellow lines in the figure).
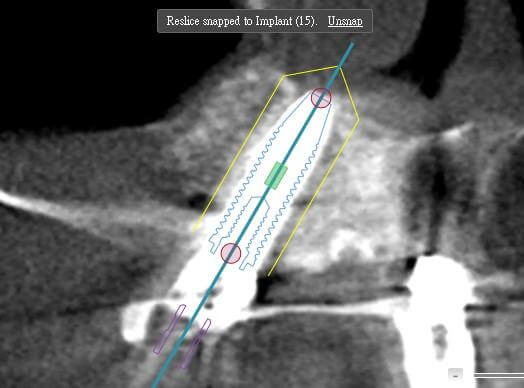
Another critical aspect is implant positioning. When working freehand, the sinus preparation should be completed first, followed by determining the implant trajectory and crestal entry point. In contrast, when using dynamic navigation, the implant path is planned preoperatively, and the procedure can be carried out according to the guided trajectory.

In this case, the patient had a history of bilateral maxillary sinusitis and was referred to an ENT specialist for FESS (functional endoscopic sinus surgery). Approximately three months after the procedure, the infection had resolved, leaving behind a thickened sinus mucosa.
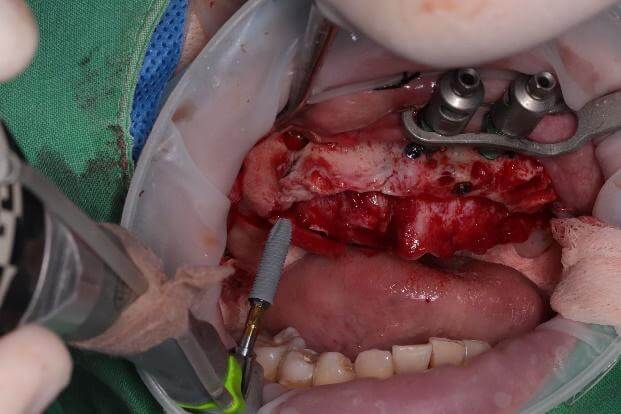
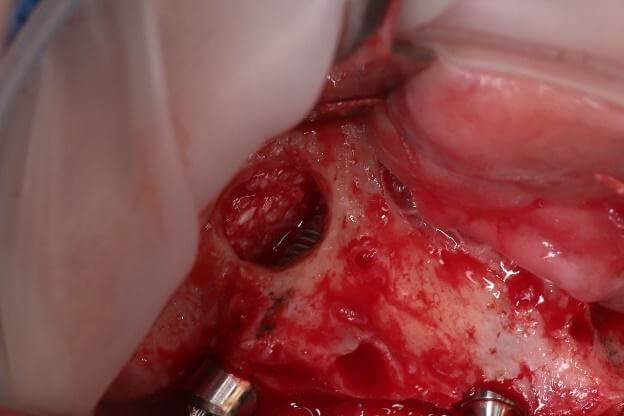
During sinus membrane elevation, the dissection was found to be quite challenging due to severe adhesions. A surgical curette was therefore used to carefully separate the membrane. After creating a triangular space (the anterior–inferior membrane), collagen was placed to protect the sinus membrane, and implant placement was then initiated.
As the implant penetrates into the sinus, a characteristic tactile feedback can be appreciated when drilling from the crestal approach: tight–loose–tight. The first layer, the crestal bone, feels firm; upon entering the sinus cavity, resistance decreases; and as the drill engages the second cortical layer, resistance increases again.
If this tactile pattern is not perceived, the implant trajectory and angulation should be promptly reassessed and corrected.
It is recommended that under-preparation of the cortical bone on the nasal cavity side be greater than at the crestal site to facilitate achieving primary stability (and avoid over-widening the apex site).

During implant placement, it is essential to ensure that the implant apex engages the second layer of cortical bone; otherwise, the implant may spin without achieving stability. Once the implant is fully seated and adequate insertion torque is confirmed, placement is complete.
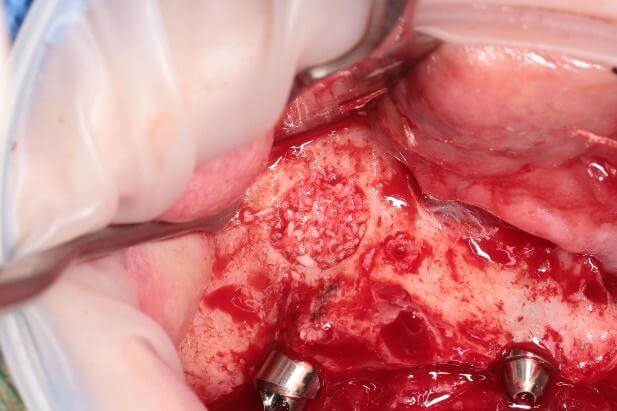
The sinus cavity is then filled with bone graft material. However, grafting may not be necessary if at least 8 mm of bone engagement is achieved. In this case, only about 2 mm of bone engagement was present at both ends, so bone grafting was performed.
Another important consideration is implant selection. The number of systems available on the market suitable for trans-sinus procedures is quite limited, with implant length being the primary constraint.
In this case, the patient was a petite female, and a 15 mm implant was used. For larger patients or male patients, implant lengths of 20–25 mm are more common.
In addition, the implant design should emphasize engagement as the main source of stability, which increases the likelihood of achieving good primary stability. The relationship between the apex diameter and the implant body diameter is also an important consideration.
There are many technical details involved—if you’re interested, we can go through them step by step during the course.
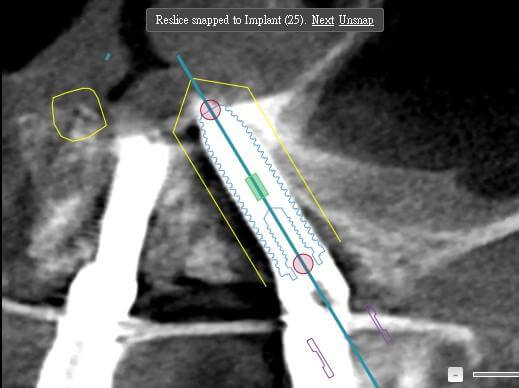
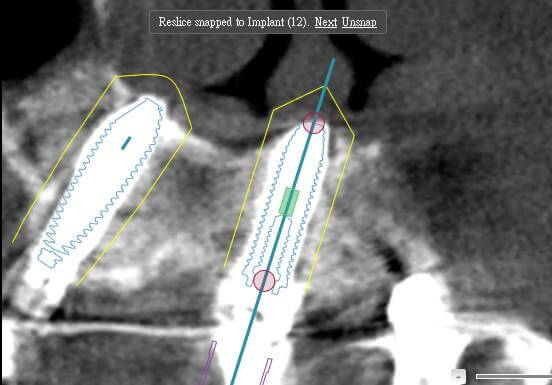 Figure 10: Implant #12 engaging the vomer bone for stability.
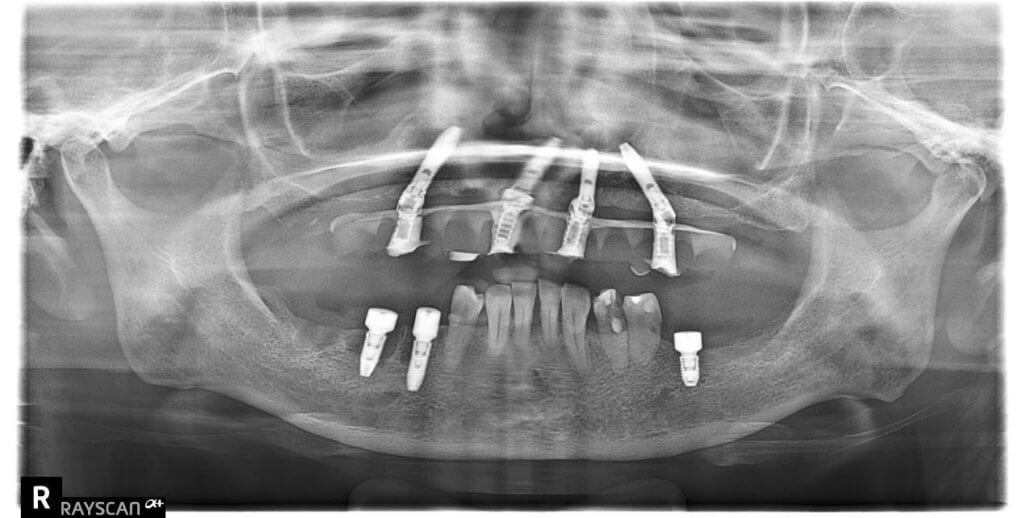
Figure 10: Implant #12 engaging the vomer bone for stability.Below are the postoperative photographs and radiographs.