1. Patient Condition Overview
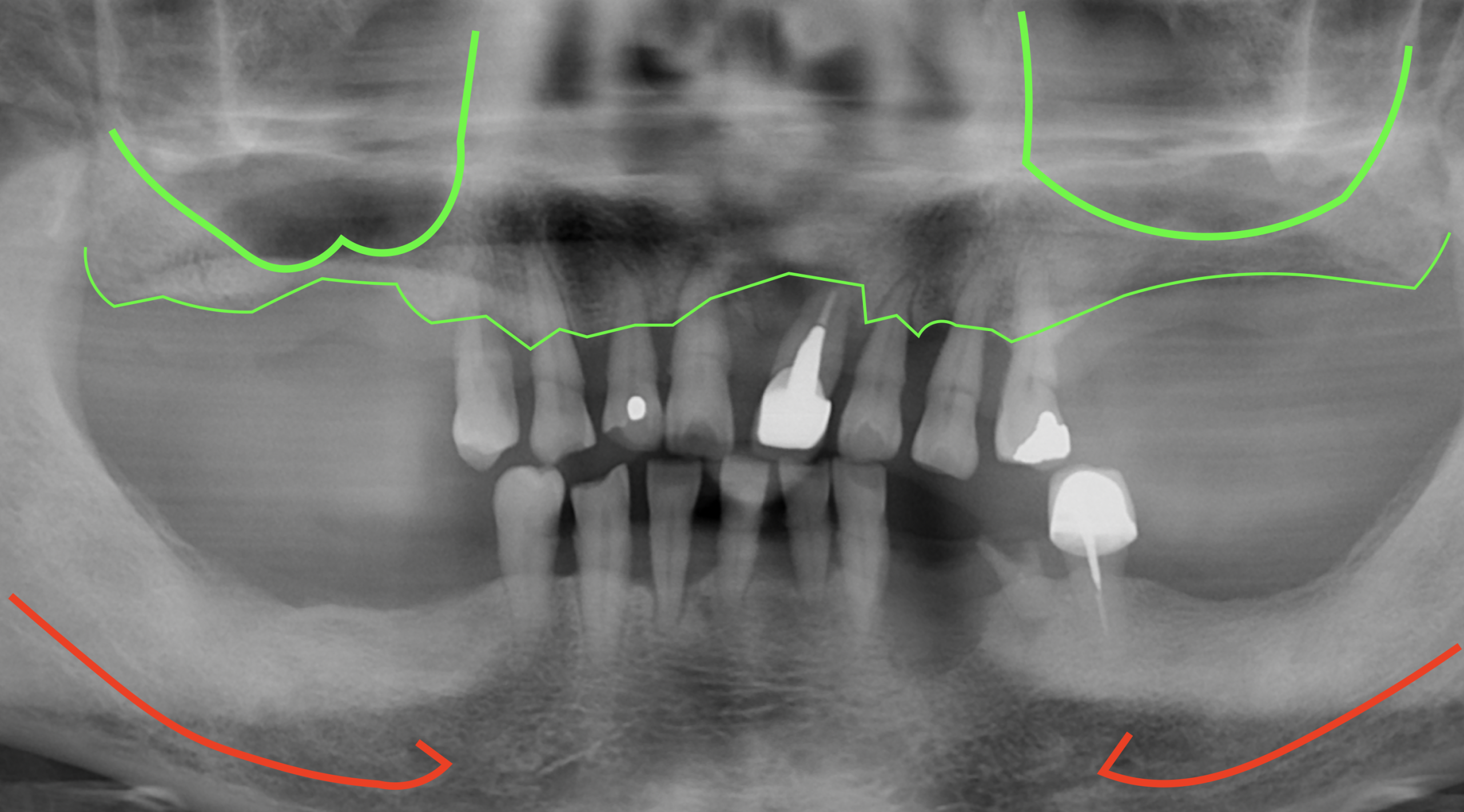
A 62-year-old male patient presented with complaints of mobile teeth and expressed a desire to improve masticatory function.
After discussing the treatment plan with the patient, full-arch rehabilitation using the All-on-X approach for both the maxilla and mandible was recommended.
In the maxilla, bone volume in the anterior region (positions 6) was limited; however, the bone quality in the tuberosity area was favorable.
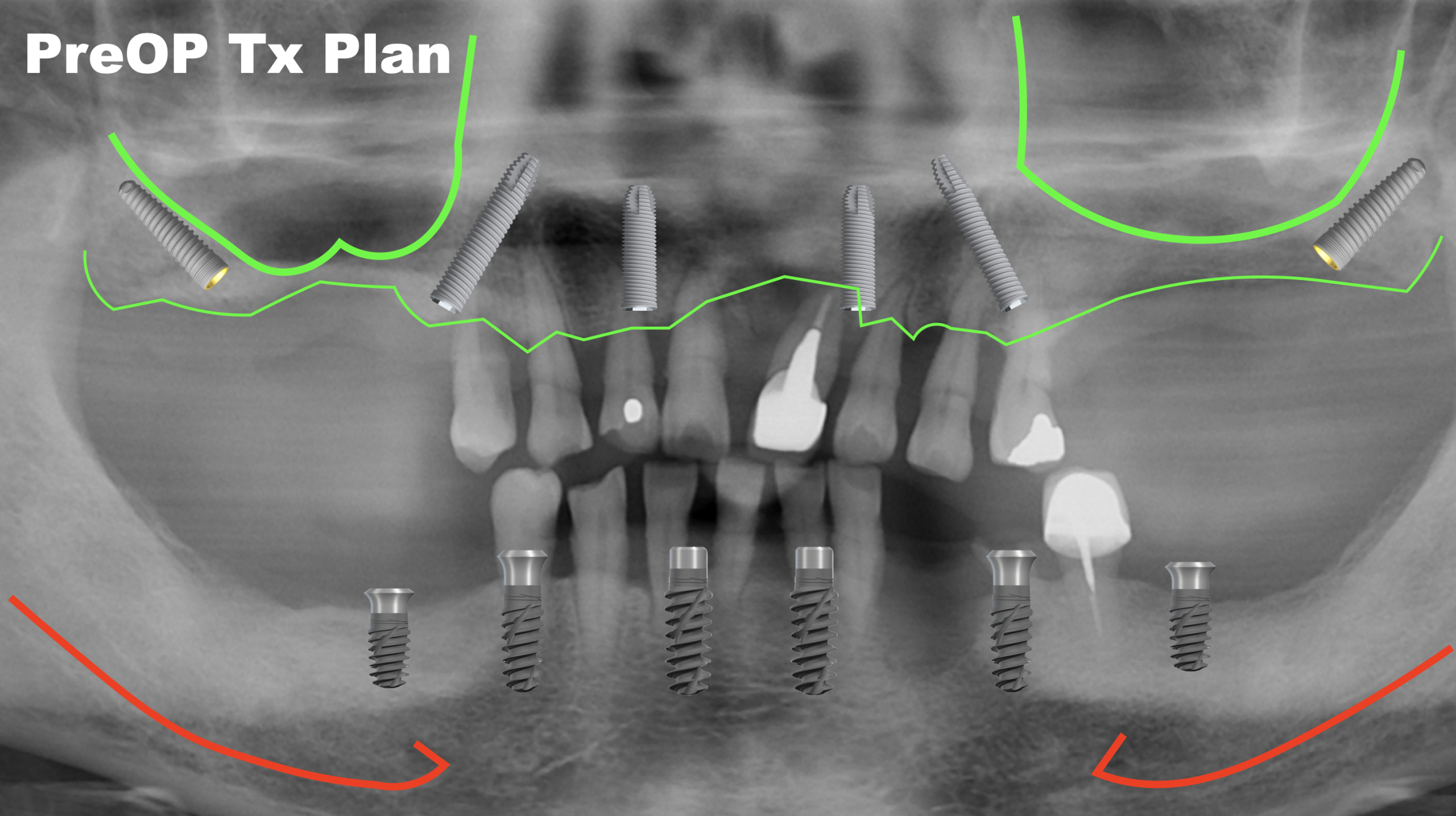
2. Treatment Plan
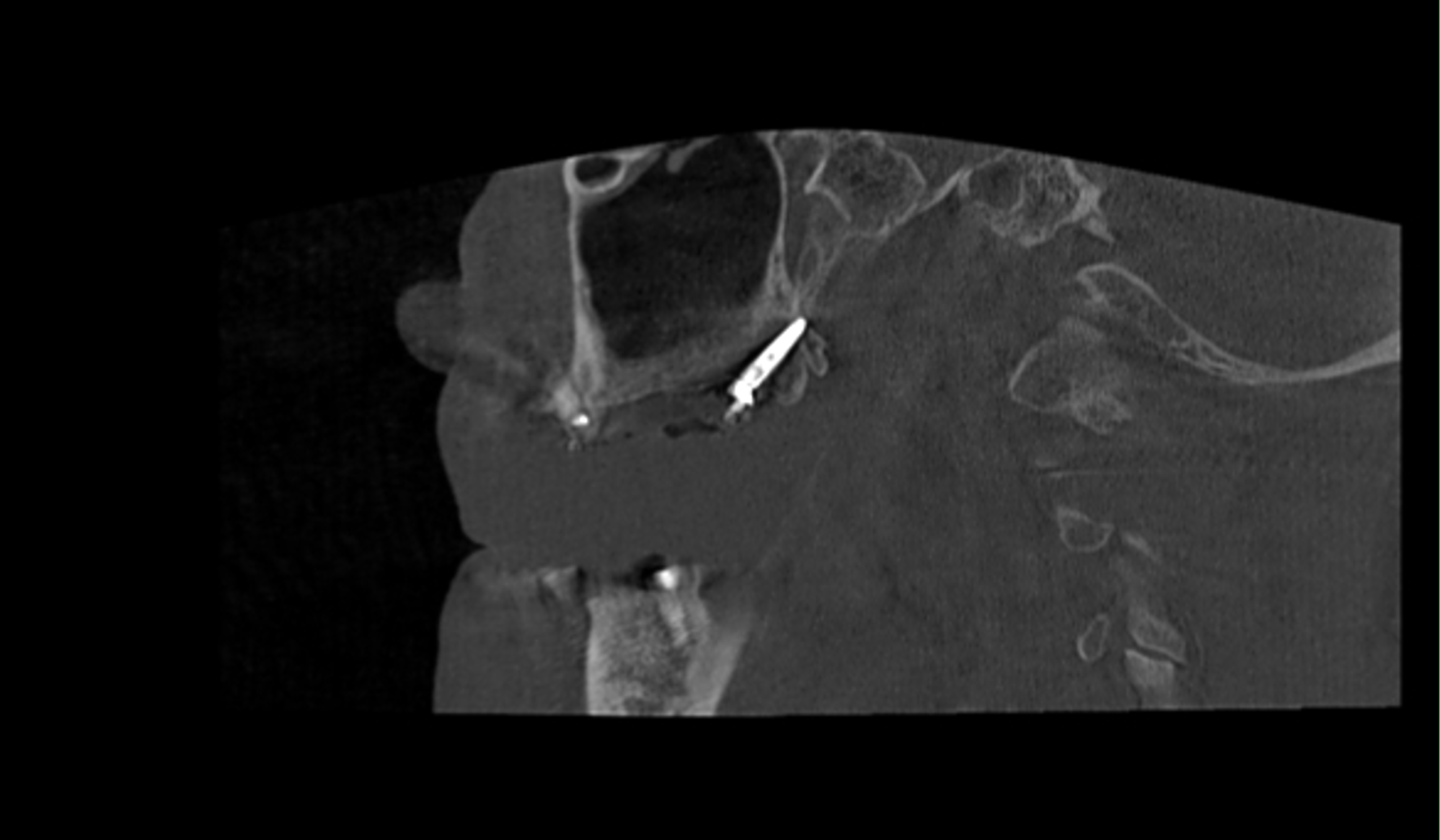
For the maxilla, an All-on-6 approach will be performed, including two pterygoid implants.
According to the PATZi classification, this case is categorized as P1A1T1Z0.
In the mandible, bone volume is sufficient to allow full-arch rehabilitation using tissue-level implants. Implant placement will aim for optimal parallelism so that an immediately loaded provisional prosthesis can be designed as a screw-retained, splinted denture.
After three months, once osseointegration is achieved, the definitive prosthesis can be fabricated and divided into three segments: 44–46, 43–33, and 34–36.
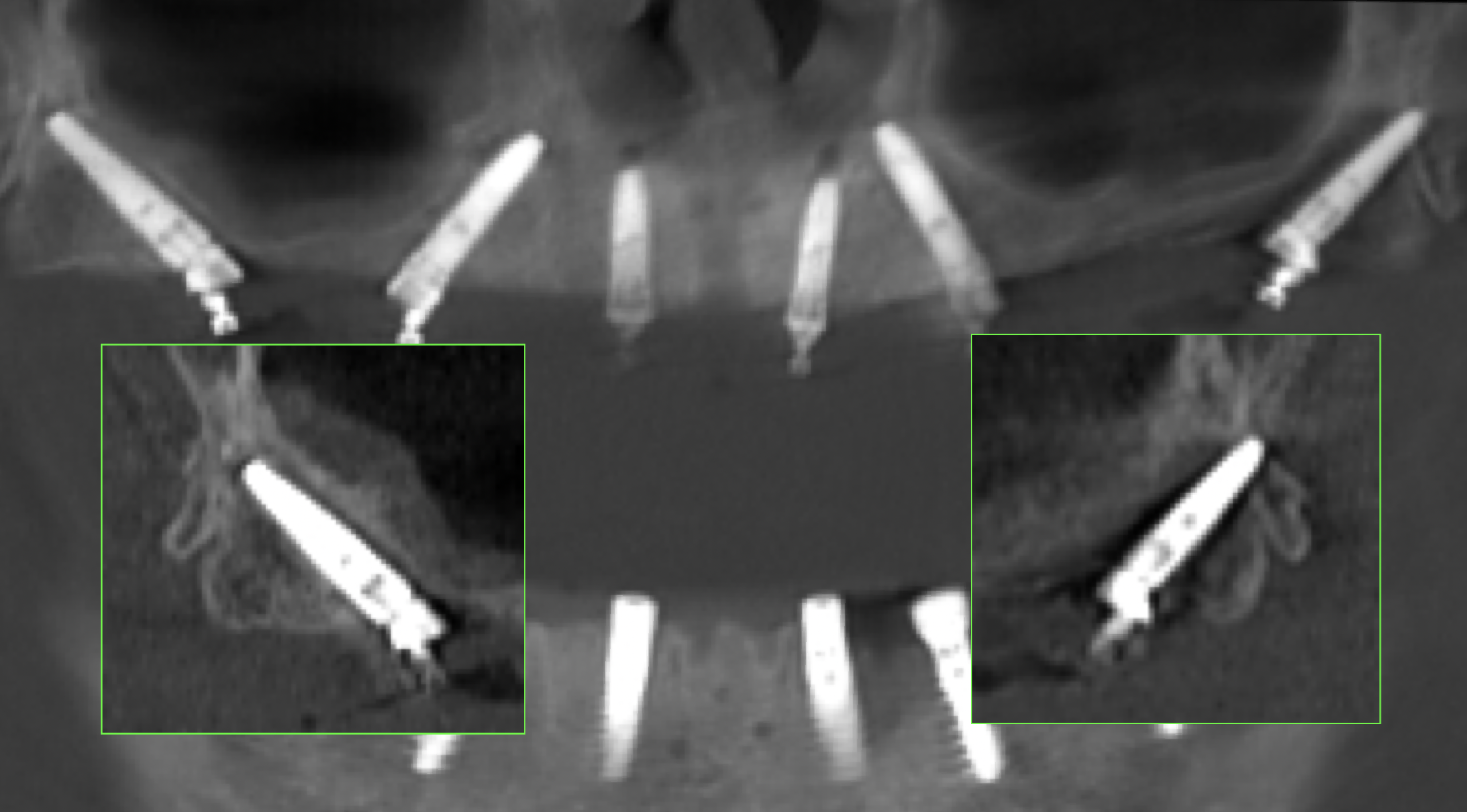
▍Using X-guide navigation, nearly parallel implant angulations can be achieved.
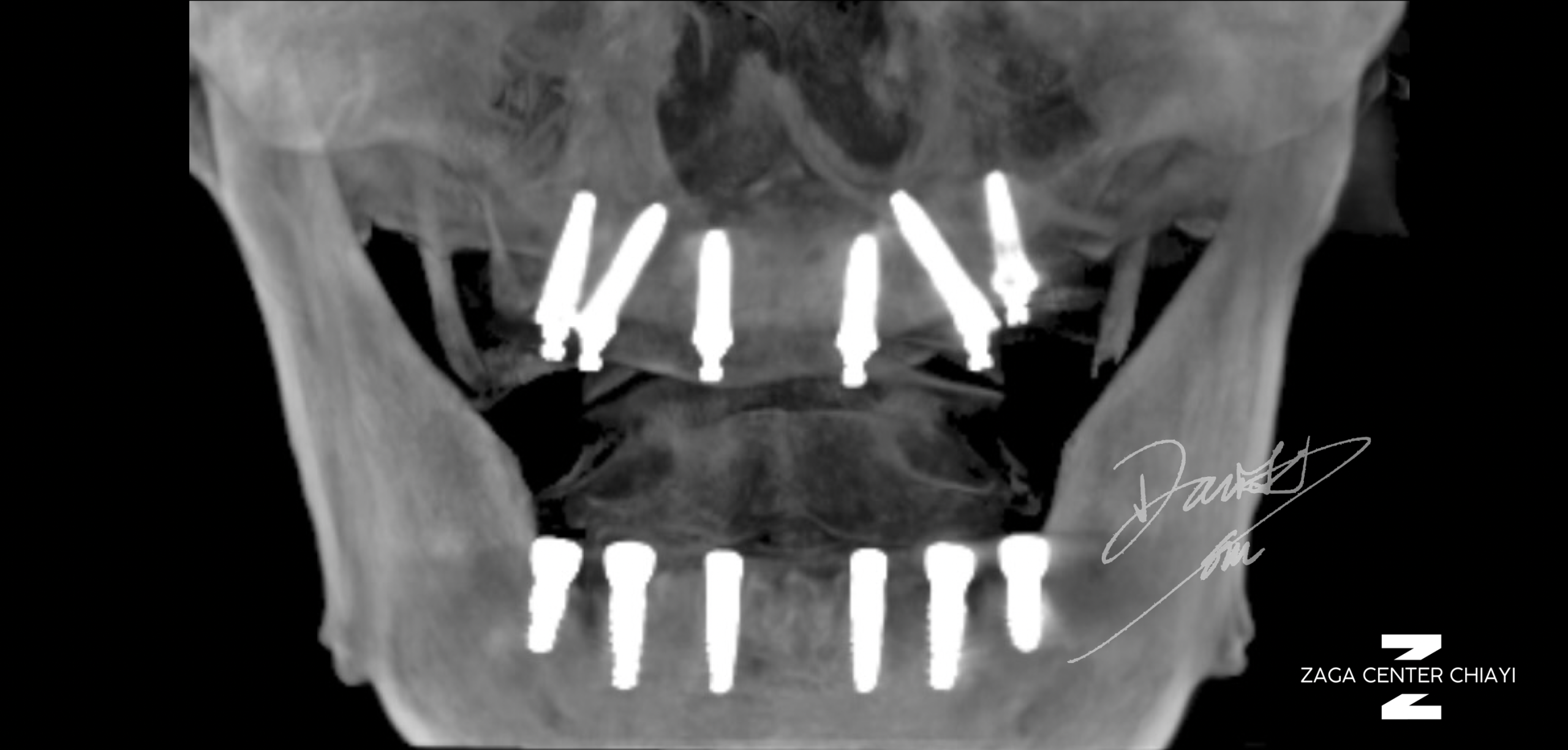
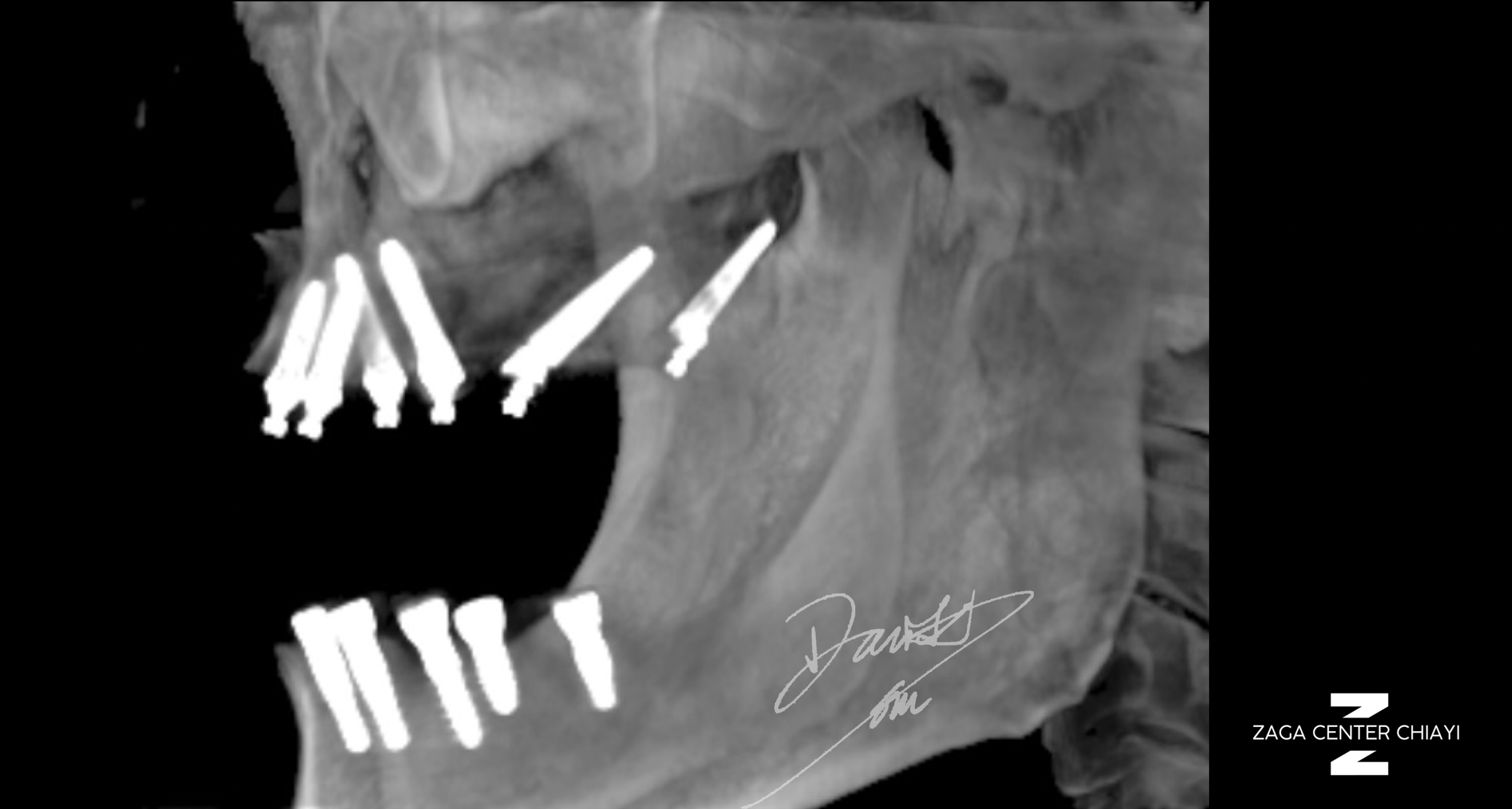
▍By performing surgery with navigation guidance, implant placement can closely follow the contour of the sinus, allowing precise positioning at the intended target site.
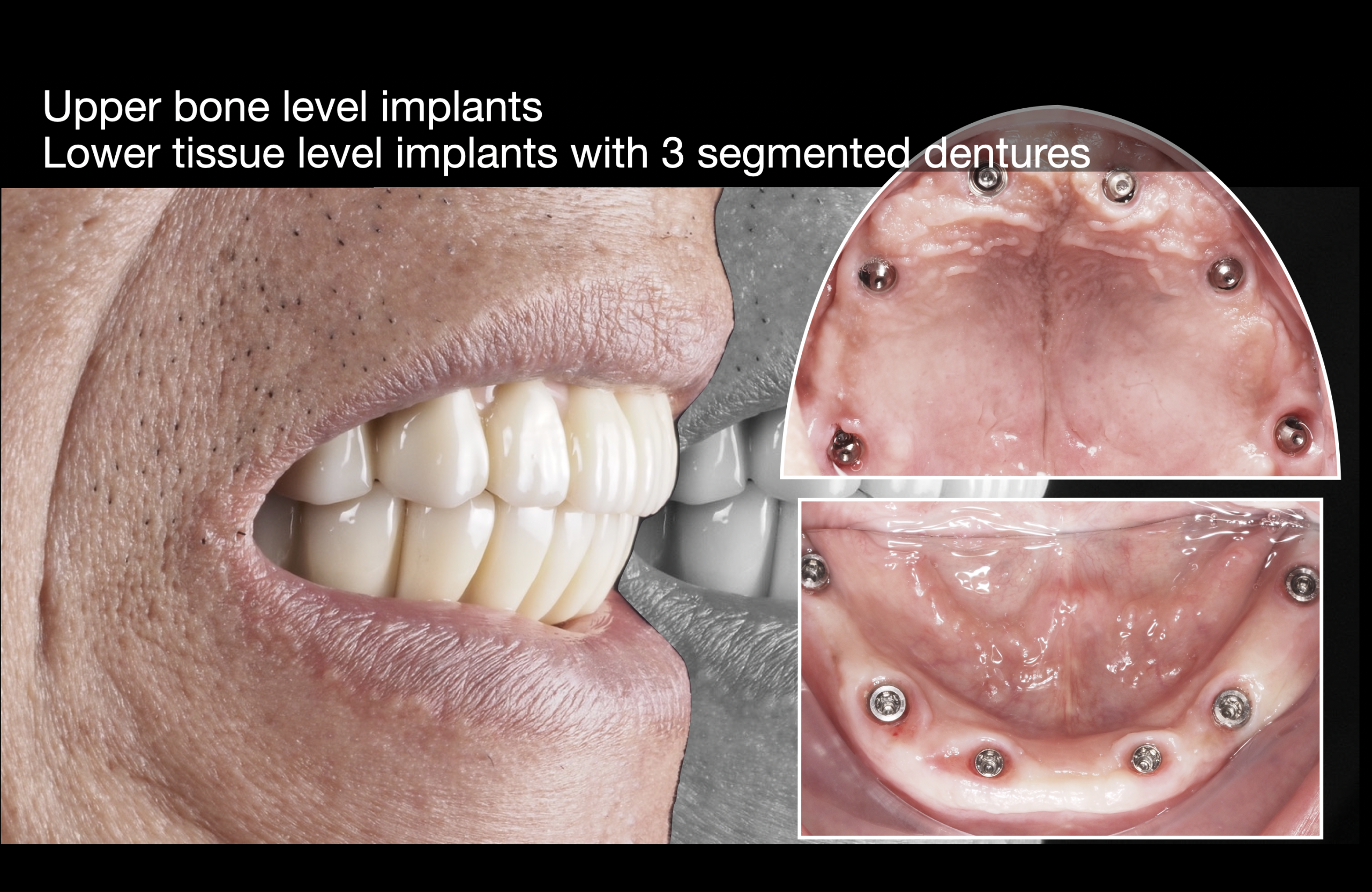
▍The maxillary prosthesis can be designed as a one-piece restoration. At the connection with the MUA, a non-submerged Ti-base is used. The intaglio surface is designed to be convex to facilitate hygiene and ease of cleaning.

▍Intraoral and extraoral views show that sufficient keratinized gingiva (KG) has been preserved.
3. Treatment Outcomes and Insights
(1)
The use of X-guide enables precise implant placement; this case serves as a good demonstration of its accuracy.
(2)
All-on-X with tissue-level implants:
1.Favorable bone conditions are required, allowing placement of at least 7.0 mm implants in the posterior region. Additionally, implants at positions 34 and 44 should be placed straight (without the need for tilted implants).
2.Typically designed as FP1, so bone conditions should not be compromised. The restorative space is maintained at approximately 10–13 mm, with about 10 mm from bone level in the posterior region.
3.Bone leveling is necessary because tissue-level implants essentially determine the MUA height during placement, leaving no flexibility for vertical adjustment afterward.
4.These conditions are generally achievable only in the mandible. In the maxilla, due to divergent bone anatomy, achieving consistent implant angulation is more difficult.
5.This approach allows for immediate loading with a screw-retained splinted denture. The definitive prosthesis can be fabricated similarly to conventional 3-unit bridges, which facilitates easier hygiene maintenance.