1、Introduction
Dynamic navigation implantology enables precise transfer of prosthetically driven preoperative planning into real-time intraoperative guidance. During surgery, the entry point, angulation, and depth of the drill and implant can be continuously monitored, enhancing the predictability of implant placement.
For fully edentulous or full-arch reconstruction patients, conventional surgical guides often lack stability due to the absence of tooth support and may even require additional fixation with bone screws, increasing surgical invasiveness and wound burden.
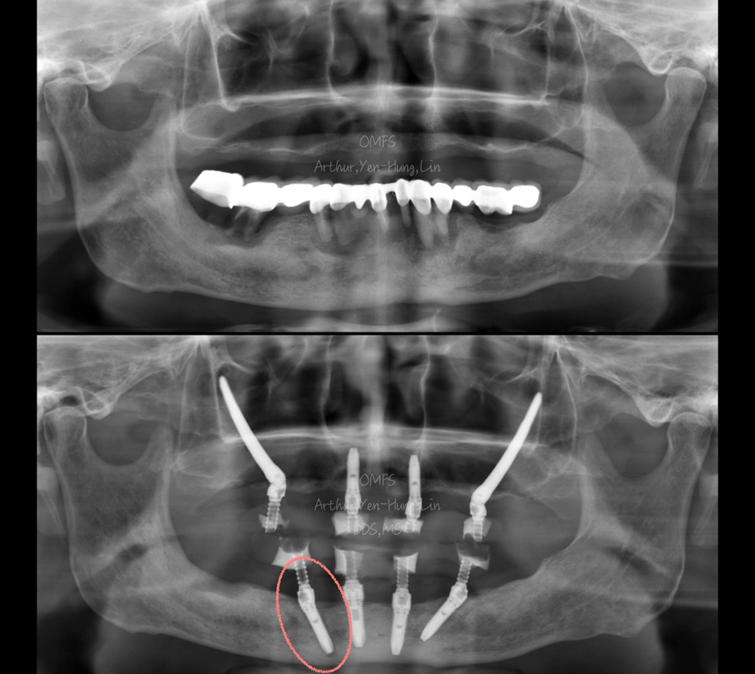
This case report demonstrates how, following full-arch reconstruction, a failed osseointegration of an implant in the right mandibular posterior region was managed. By utilizing the X-Guide dynamic navigation system in combination with a customized device anchored to previously successful implants, a rescue re-implantation of tooth #45 was performed. This approach aimed to minimize surgical trauma, shorten recovery time, and reduce the need for prosthetic adjustments.
2、Patient Condition Overview
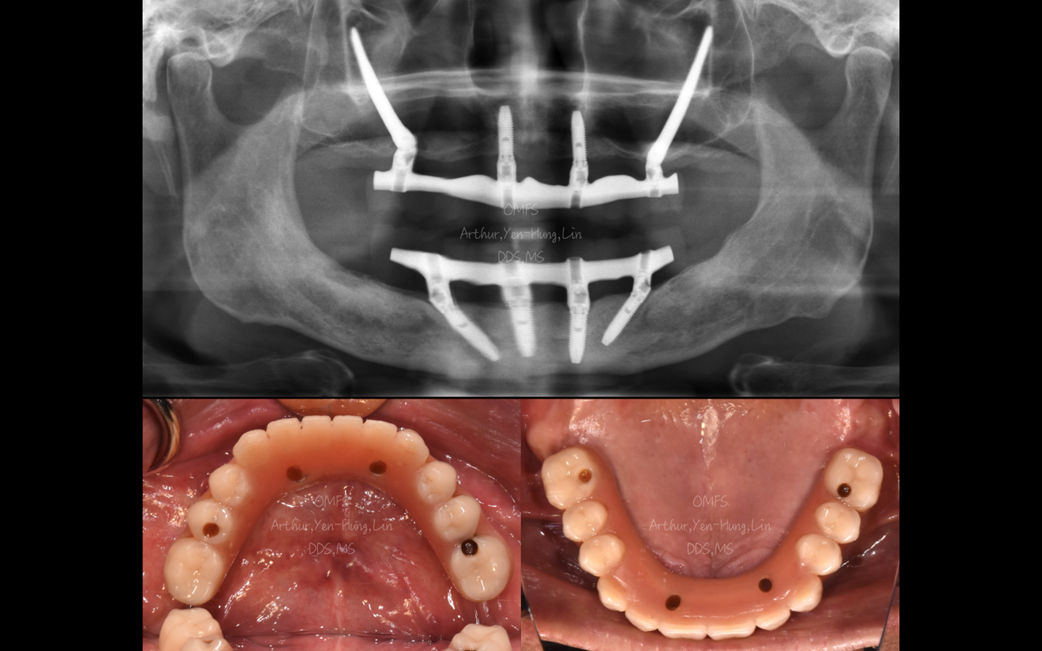
The patient is a 67-year-old male with a medical history of hypertension and diabetes mellitus. Intraoral examination revealed missing teeth in the maxilla and severe periodontitis in the mandible. Approximately three months after completion of full-arch reconstruction of both jaws, follow-up examination showed failure of osseointegration of the implant at site #45 in the right mandibular posterior region.
3、Treatment Plan
Considering that the patient had already entered the full-arch reconstruction phase and wished to minimize the invasiveness of a secondary surgery, a single-implant rescue re-implantation strategy was adopted:
Two successfully osseointegrated implants in the mandibular anterior region were utilized as anchorage bases.
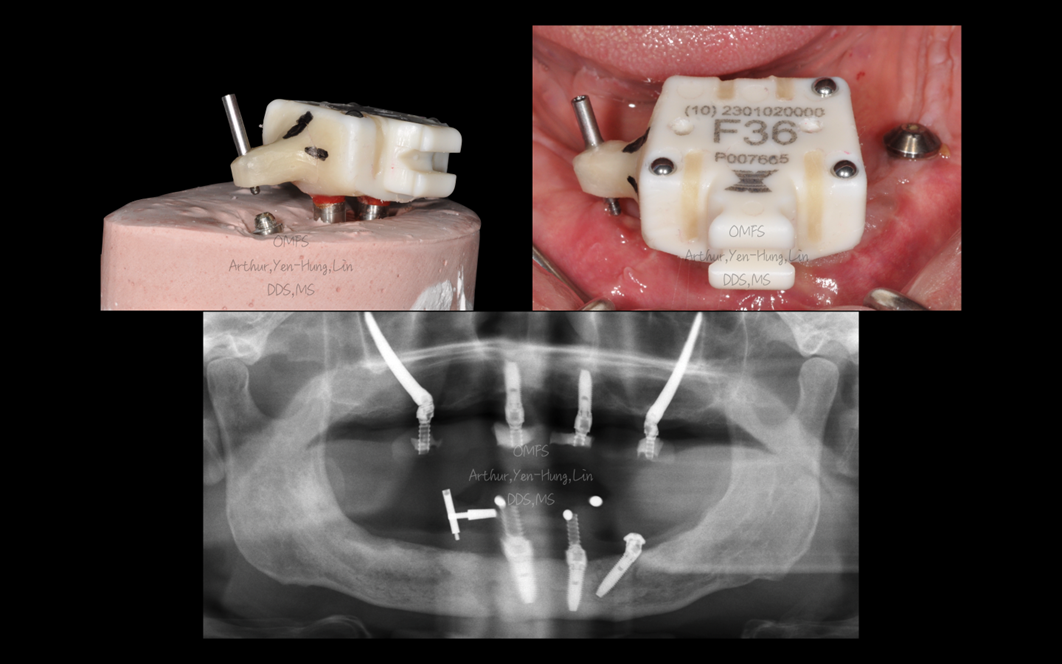
A screw-retained, customized X-Clip was fabricated to provide stable reference for dynamic navigation.
Using this setup, re-implantation at site #45 was completed without the need for additional bone screw fixation, allowing for a smaller incision while preserving the design of the existing provisional prosthesis.
▍Surgical Design and Preoperative Preparation
1) Design of the Customized X-Clip
Preoperatively, the technician was instructed to fabricate the X-Clip based on the spatial relationship between the X-Clip and the two implants in the mandibular anterior region. A screw-retained, repositionable customized X-Clip was thus created. Since the patient had an existing provisional prosthesis, the original model/data could be directly utilized for fabrication, reducing the time and cost associated with re-impression and reconstruction procedures.
2) Prosthetically Driven Planning for #45
The implant position and the orientation of the multi-unit abutment (MUA) at site #45 were planned based on the existing provisional prosthesis design. This prosthetically driven approach allowed restoration of function with minimal modification to the provisional prosthesis after surgery.
3) Localization of the MUA Screw Hole
To facilitate intraoperative verification of the MUA screw hole direction and position, a guide pin concept was incorporated into the planned #45 region. This served as a reference point during surgery, ensuring that the implant axis closely aligned with the prosthetic screw access hole.
▍Surgical Procedure and Intraoperative Key Points
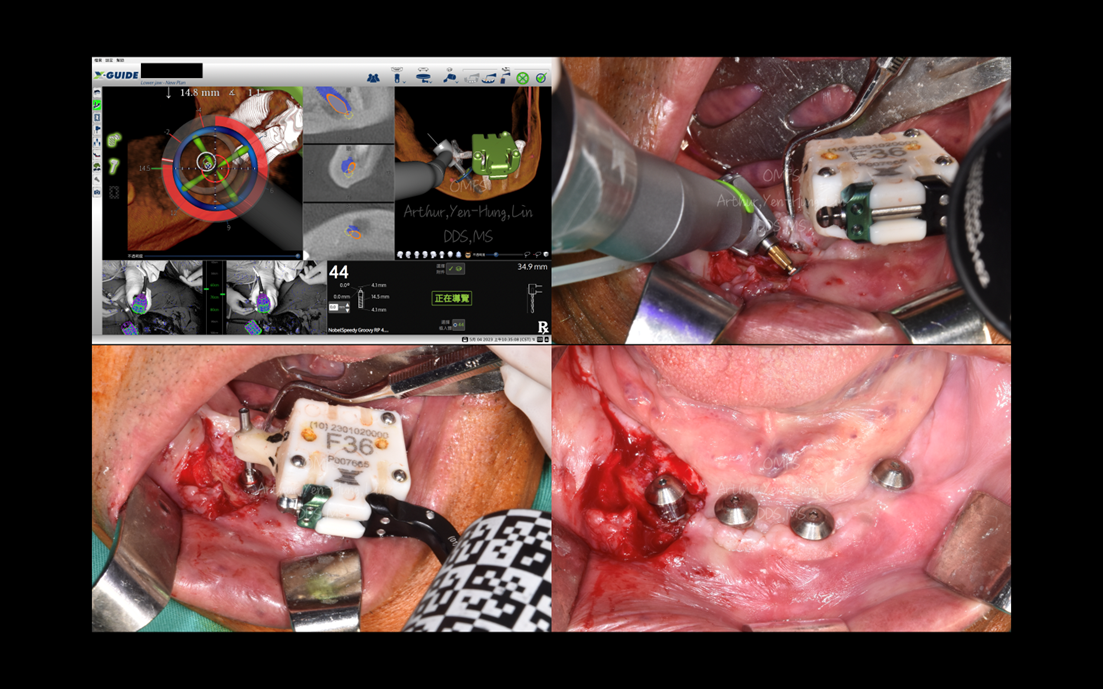
During surgery, the customized X-Clip was first secured with screws onto the two successfully osseointegrated implants in the anterior mandible. After completing system calibration, osteotomy preparation and implant placement were performed under real-time guidance using the X-Guide dynamic navigation system, following the preoperative plan.
The key advantages of this approach include:
Stable reference fixation: The X-Clip is anchored to existing successful implants, providing a reliable reference for positioning and tracking.
Reduced incision and flap elevation: Minimizes unnecessary extensive flap reflection in the posterior region, thereby reducing soft tissue trauma.
Avoidance of additional bone screws: Eliminates the need for extra fixation screws for surgical guides or reference frames, reducing invasiveness and postoperative discomfort.
Improved accuracy of implant positioning: Dynamic navigation allows real-time adjustment of angulation and depth, enabling the #45 implant to closely match the planned axis and position; the preoperative guide pin marker also assists in confirming that the MUA screw hole aligns with the original prosthetic design.
▍Facilitates Rapid Transition to Subsequent Prosthetic Procedures
Because the implant position and angulation closely match the preoperative plan, most of the original provisional prosthesis design can be preserved. Postoperatively, only minor modification—specifically, creating a new access hole at site #45—is required to reinsert the provisional prosthesis and restore the intended function and occlusal scheme. This significantly reduces the need for prosthesis remaking and shortens chair time and follow-up visits.
4. Conclusion
For fully edentulous or full-arch reconstruction patients, when a single implant fails to achieve osseointegration, performing a rescue re-implantation using the X-Guide dynamic navigation system represents a well-structured, minimally invasive, and highly predictable solution.
By utilizing a customized X-Clip anchored to previously successful implants as a stable reference, this approach not only minimizes surgical trauma and eliminates the need for additional bone screws, but also allows implant placement to closely follow prosthetically driven planning. Furthermore, the original provisional prosthesis can be largely preserved with minimal modification, thereby enhancing patient comfort and overall treatment efficiency.