此篇是 ITI Consensus Workshop,第一次針對 Zygoma implant 編寫共識會議指引。
▋ 前言
Zygoma implant主要適用於上顎骨萎縮或不足的病例。平均追蹤時間為75.4個月(6.3年)的情況下,長期平均Zygoma implant的存活率為96.2%,追蹤時間為36–141.6個月(3–11.8年)。
相較於delay loading,Immediate loading統計上存活率顯著增加。在平均65.4個月的追蹤,Sinusitis的發生率為14.2%,這是導致Zygoma implant失敗最常見併發症。
此篇 ITI Consensus Workshop共識會議提出了有關規劃、手術、假牙重建、結果和以患者觀點出發的共識指引以及臨床建議。
底下節錄重點專家共識指引 。
▋ 一. 適應症 (Indications)
李醫師總結,Zygoma implant 適用於:
1.上顎骨萎縮或不足的病例
2.曾經補骨或植體失敗的病例
3.患者希望避免多次手術補骨的患者
4.接受過良性囊腫和外傷…等複雜性切除上顎骨手術患者
5.先天性上顎骨缺損,外傷及顎骨切除的替代性治療
▋ 二. 存活率 (Survival)
1. The mean survival rate between 90.3% and 100% after a follow-up of 6 months.
2. The mean survival rate of 97% (89–100%) in a mean follow-up period of 28.5 months (range 12–162 months).
3. The mean zygomatic implant survival 96.2% [95% CI 93.8; 97.7] over a mean follow-up of 75.4 months (6.3 years) with a follow-up range of 36–141.6 months (3–11.8 years).
➤ 李醫師總結
2 篇 system review 和 1 篇 meta-analysis 顯示,Zygoma implant 中長期追蹤有 90% 以上成功率。
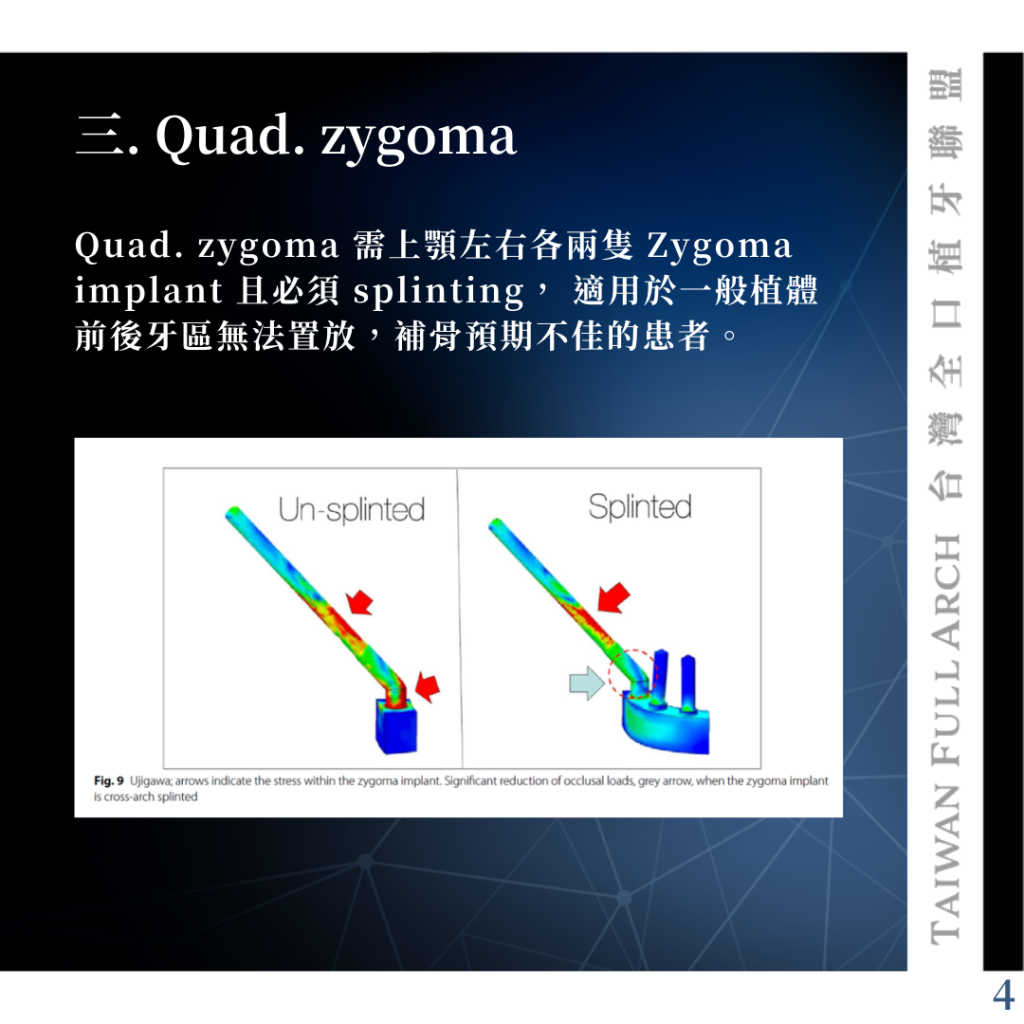
▋ 三. Quad. zygoma
Quad. zygoma 需上顎左右各兩隻 Zygoma implant 且必須 splinting, 適用於一般植體前後牙區無法置放,補骨預期不佳的患者。
▋ 四. Loading protocol (立即受力或延遲受力)
Immediate Loading protocols: were 98.1% [95% CI 96.2; 99.0] over a mean of 73.6 months follow-up.
Delayed load protocols:was 95% [95% CI 91.7; 97.1] over a mean of 69.3 months follow-up.
➤ 李醫師總結
Zygoma implant 立即受力成功率略高,但需要注意oro-antral communications 風險,李醫師建議當發生較大口鼻穿通時建議採用 delayed load protocols.
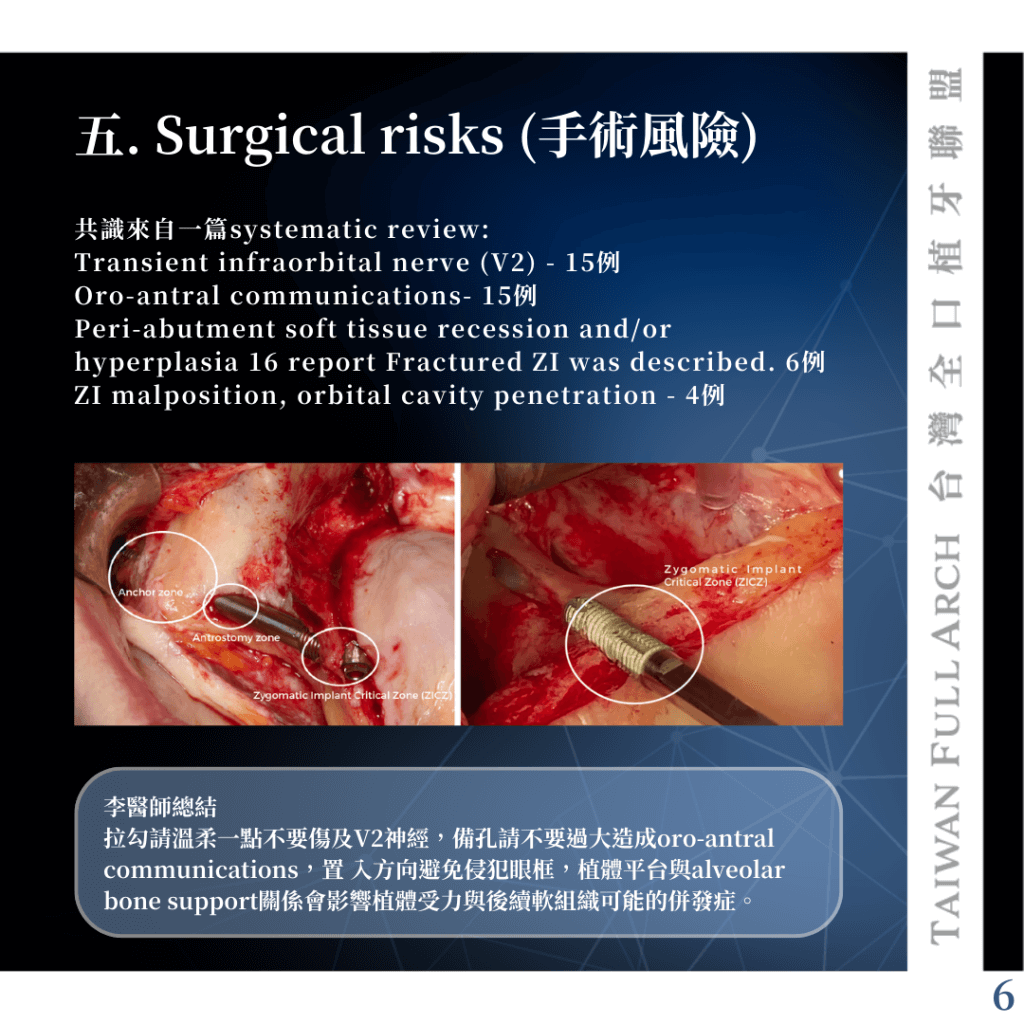
▋ 五. Surgical risks (手術風險)
共識來自一篇systematic review:
• Transient infraorbital nerve (V2) – 15例
• Oro-antral communications- 15例
• Peri-abutment soft tissue recession and/or hyperplasia 16 report Fractured ZI was described. 6例
• ZI malposition, orbital cavity penetration – 4例
➤ 李醫師總結
拉勾請溫柔一點不要傷及V2神經,備孔請不要過大造成oro-antral communications,置 入方向避免侵犯眼框,植體平台與alveolar bone support關係會影響植體受力與後續軟組織可能的併發症。
▋ 六. Failures (植體失敗)
This statement is based on a meta-analysis of 17 case series reports, which included a total of 1247 ZIsA higher failure incidence may occur within the first year (2%) compared to that of subsequent years (0.5%/year).
➤ 李醫師總結
第一年失敗率較後續幾年高,第一年失敗原因為植體本身未骨整合或不夠穩定。後續失敗原因為生物性併發症或機械性因素導致植體失敗。
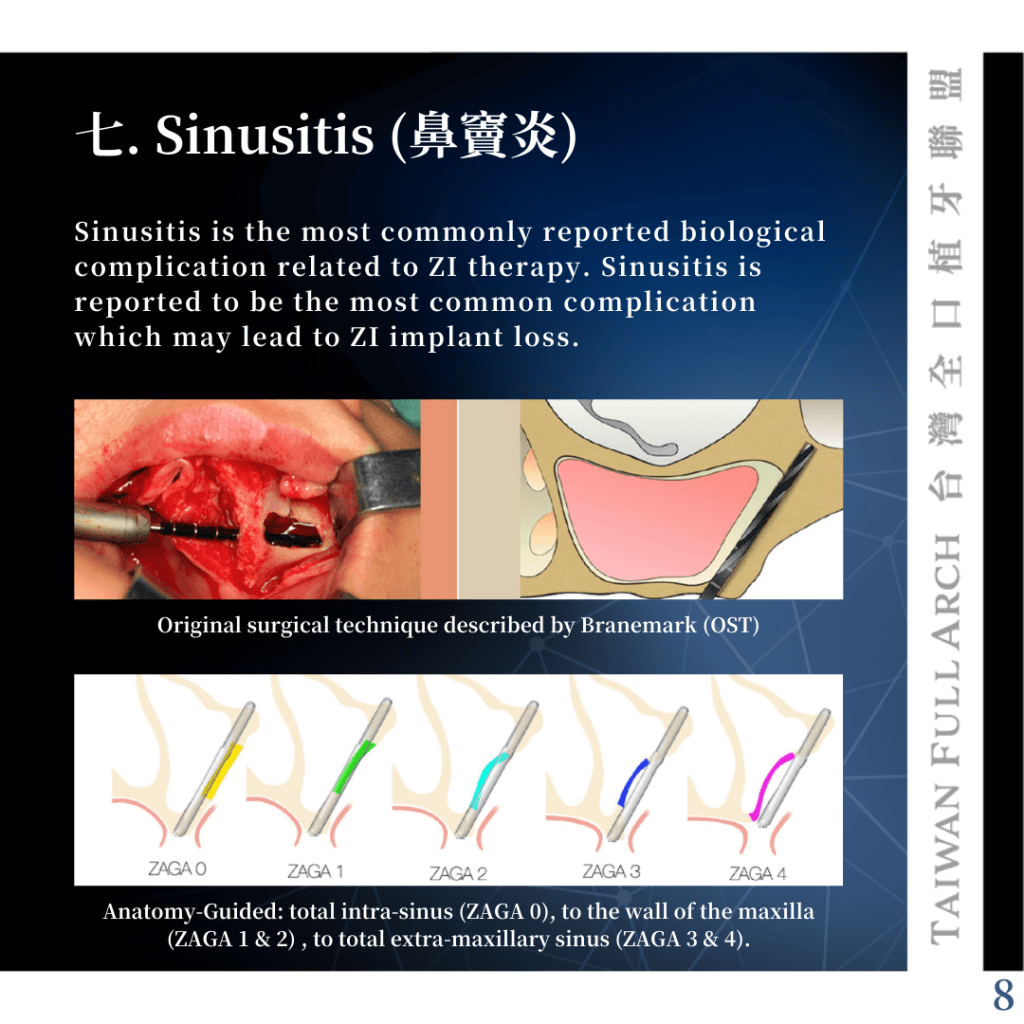
▋ 七. Sinusitis (鼻竇炎)
Sinusitis is the most commonly reported biological complication related to ZI therapy. Sinusitis is reported to be the most common complication which may lead to ZI implant loss.
➤ 李醫師總結
鼻竇炎為最常見導致 Zygoma implant 失敗的併發症,發生率從2.8% ~ 36.4% 不等。
鼻竇炎與手術技巧相關, Original surgical technique (OST) were 9.5% (0–37.5%), Anatomy- Guided were 4.4% (0–11.8%).
鼻竇炎經抗生素或合併surgical meatotomy皆可成功治療 。
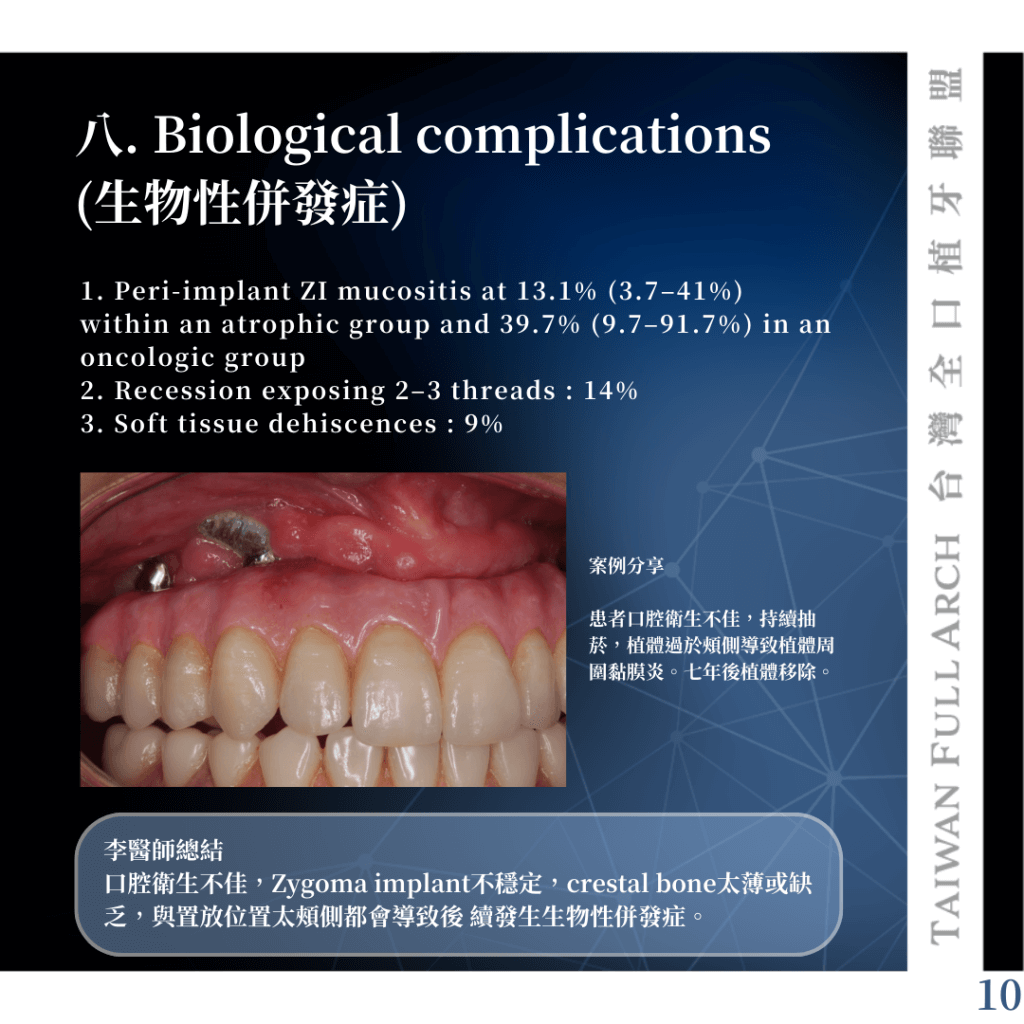
▋ 八. Biological complications (生物性併發症)
1. Peri-implant ZI mucositis at 13.1% (3.7–41%) within an atrophic group and 39.7% (9.7–91.7%) in an oncologic group
2. Recession exposing 2–3 threads : 14%
3. Soft tissue dehiscences : 9%
➤ 李醫師總結
口腔衛生不佳,Zygoma implant不穩定,crestal bone太薄或缺乏,與置放位置太頰側都會導致後 續發生生物性併發症。
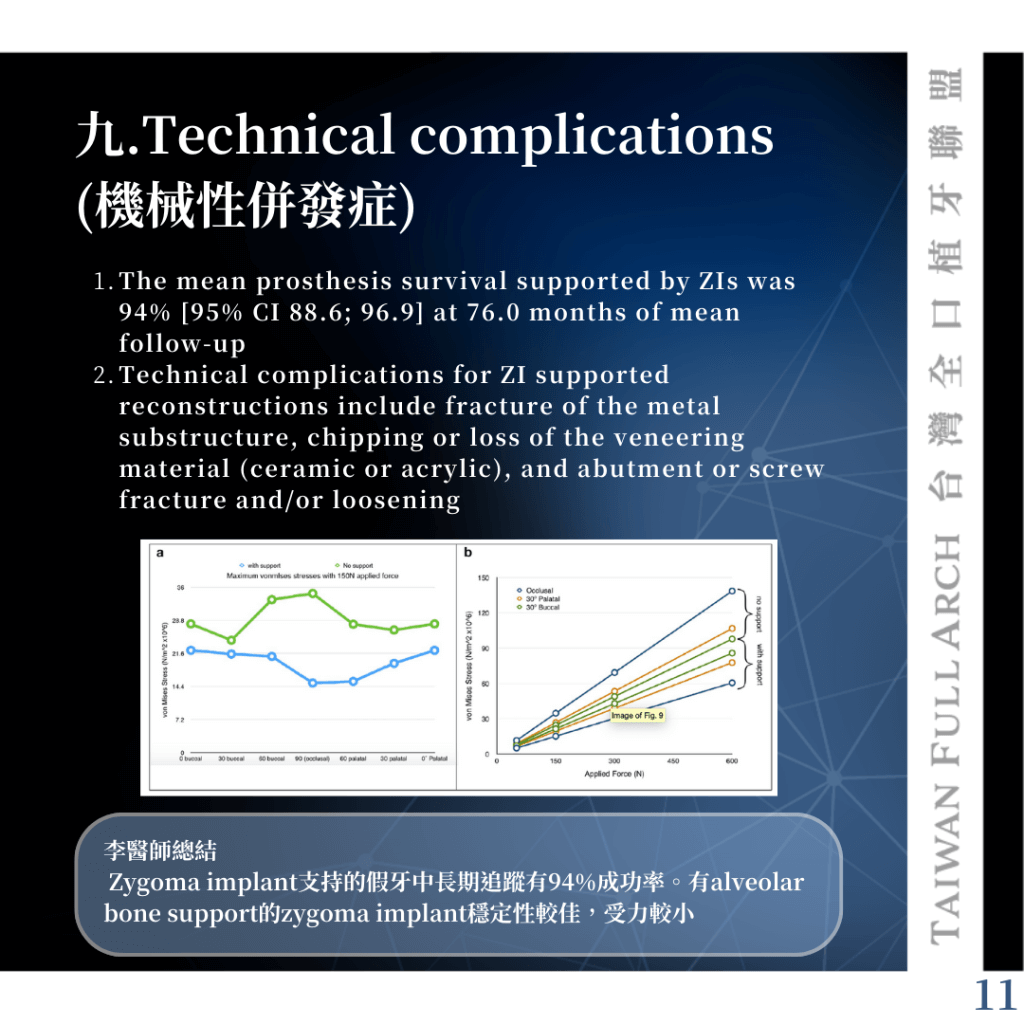
▋ 九.Technical complications (機械性併發症)
1.The mean prosthesis survival supported by ZIs was 94% [95% CI 88.6; 96.9] at 76.0 months of mean follow-up.
2.Technical complications for ZI supported reconstructions include fracture of the metal substructure, chipping or loss of the veneering material (ceramic or acrylic), and abutment or screw fracture and/or loosening.
➤ 李醫師總結
Zygoma implant支持的假牙中長期追蹤有94%成功率。有alveolar bone support的zygoma implant穩定性較佳,受力較小
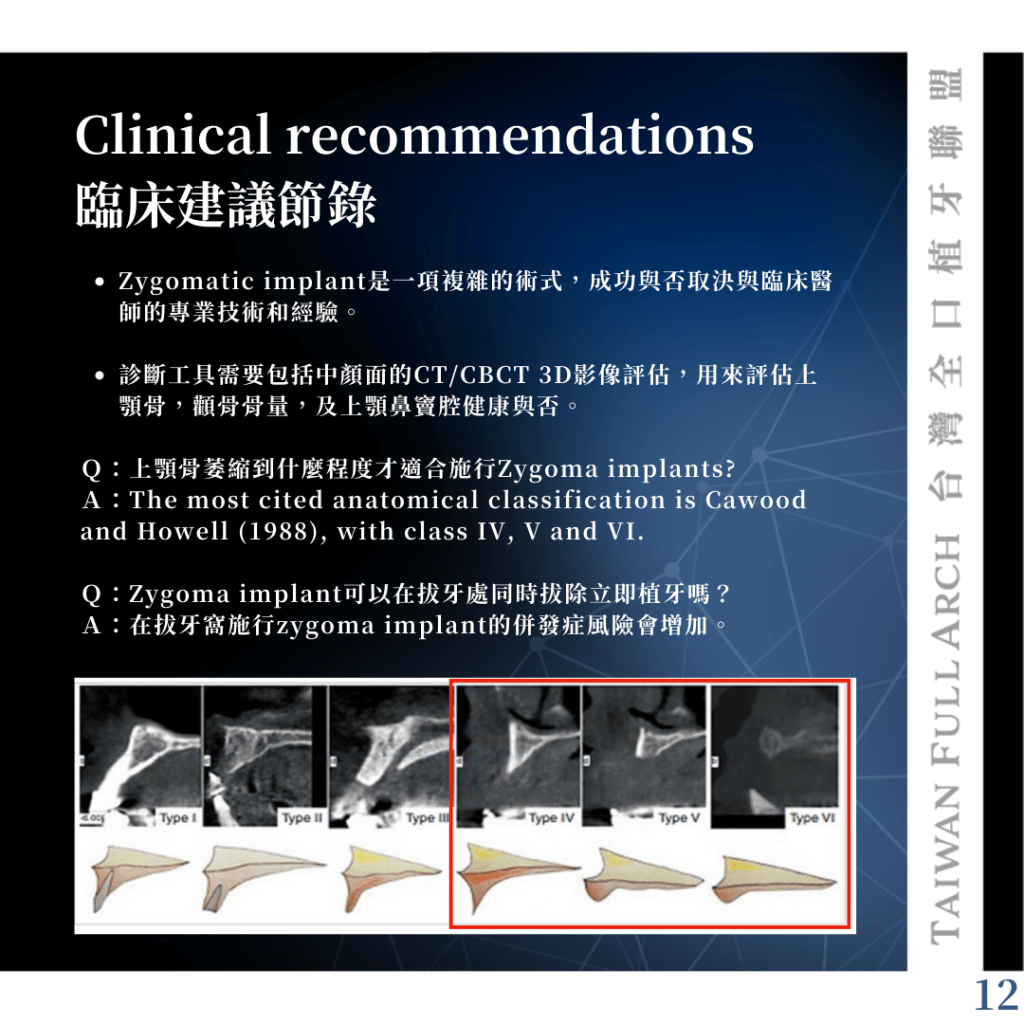
▋ Clinical recommendations 臨床建議節錄
• Zygomatic implant是一項複雜的術式,成功與否取決與臨床醫師的專業技術和經驗。
• 診斷工具需要包括中顏面的CT/CBCT 3D影像評估,用來評估上顎骨,顴骨骨量,及上顎鼻竇腔健康與否。
Q:上顎骨萎縮到什麼程度才適合施行Zygoma implants?
A:The most cited anatomical classification is Cawood and Howell (1988), with class IV, V and VI.
Q:Zygoma implant可以在拔牙處同時拔除立即植牙嗎?
A:在拔牙窩施行zygoma implant的併發症風險會增加。
Q:導引手術及導航手術在Zygoma implant的角色與地位?
A:即使有導引手術輔助,直接肉眼目視仍然很重要,可以避免發生解剖構造侵犯的併發症。
Q:針對Zygoma implants的全口重建治療,有何特殊挑戰需要特別去面對?
A:Zygomatic implants 重建需要更高標準去維護(李醫師補充:因外側骨頭薄或沒有,靠近鼻竇腔,植體長較容易些微晃動)。其咬合力量大小也有局限性( 意謂著咬合力過強的患者可 能不適合接受zygoma implant治療)。患者也需要了解後續併發症的處理也較一般植牙複雜。